MATERNAL ARREST: ANESTHESIA GUIDE PDF
Key points in Maternal Codes:
If no ROSC in 4 minutes – Emergent crash C/S no matter where you are – could be in L&D room, hallway, OR, PACU, CT scanner, triage bay, in a bed or on the floor -the literal floor. PERIMORTEM C/S OCCURS AT SITE OF ARREST. DO NOT MOVE PATIENT.
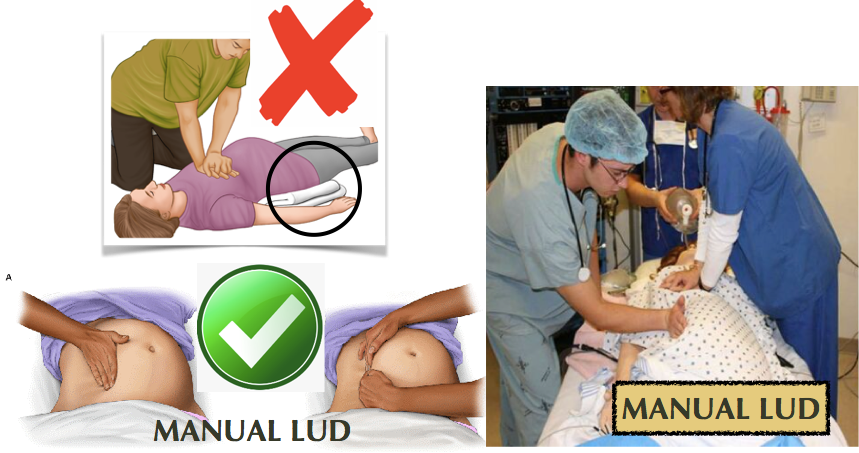
Leave patient supine & flat during CPR. A firm backboard should be used to improve compression quality. Use manual left uterine displacement. DO NOT tilt the backboard. DO NOT use blanket/roll under left hip. (The 30 degree tilt decreases force & effectiveness of chest compressions. [AHA, 2015]) . ALL IVs UPPER extremities ONLY. HUMERUS IntraOsseous line if necessary.
BEGIN CRASH C/S AT 4 MINUTES, FETUS DELIVERED BY 5 MINUTES
C/S is to facilitate Maternal CPR & resuscitation for maternal survival, not for fetal benefit, although < 5mins from arrest to delivery has improved fetal outcomes.
- Transverse or vertical incision (whatever OBGYN feels they are faster at), placenta can stay in situ until ROSC, abdomen can be packed and stapled until ROSC.
- Emergent c/s only considered if fetus > ~22-24 wks, as prior to this, fetal gestational size is not large enough to compromise maternal circulation in CPR (primary concern), and viability is unlikely, so best outcome is just restored maternal perfusion to restore fetal perfusion.
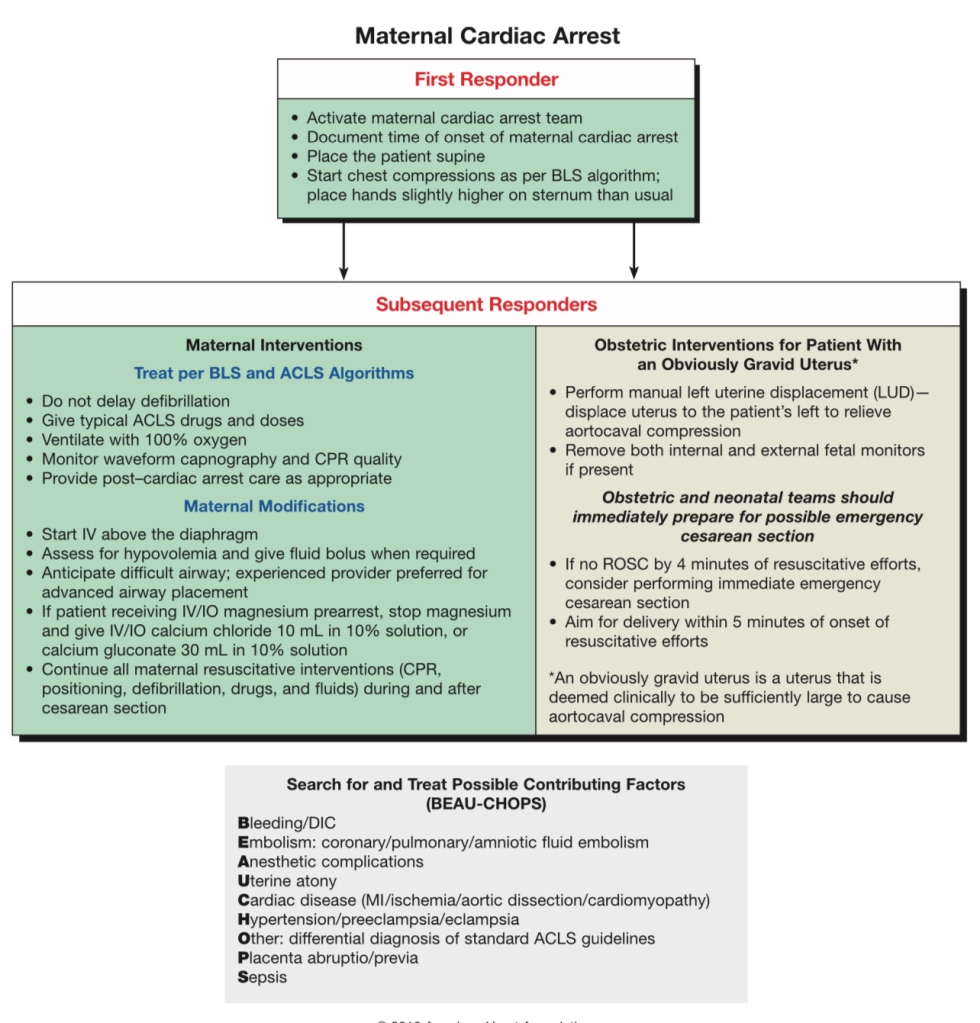
Maternal Cardiac Arrest Algorithm:
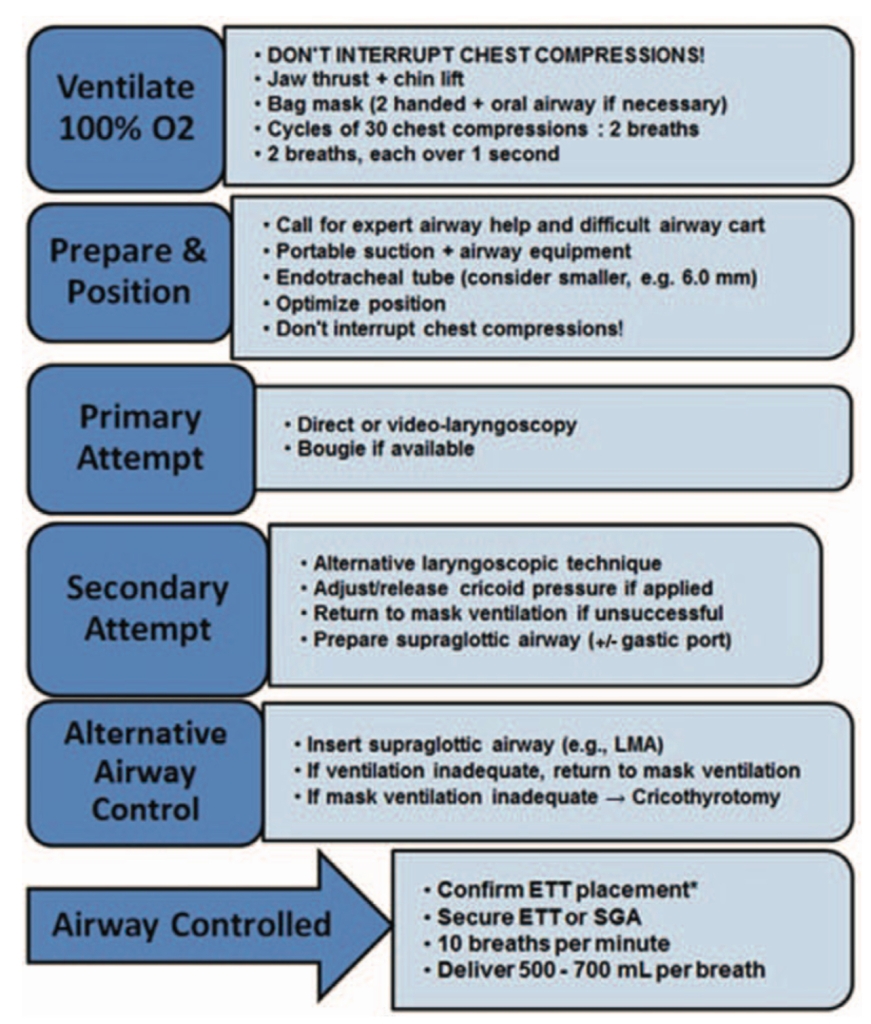
SOAP algorithm for Airway Management during CPR:
61. Case Report: Cardiac Arrest due to Peripartum Cardiomyopathy – Medical College of Wisconsin
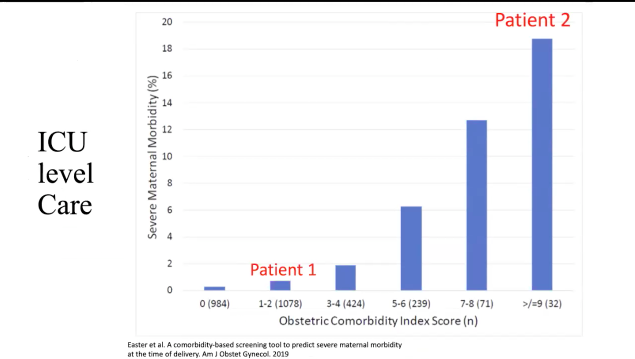
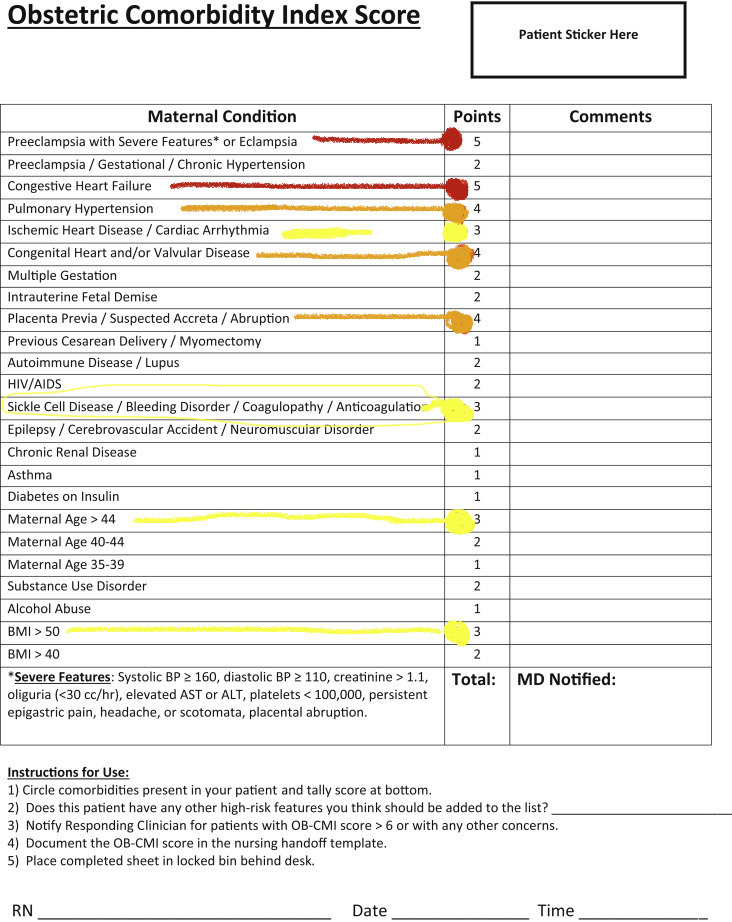
The big players in maternal morbidity …cardiac is huge risk:
- Index score for comorbidities
- Bar graph showing totals and morbidity%
How these comorbidities contribute to requiring ICU-level care: