PRETERM CONSIDERATIONS
- No Latex gloves used in spinals, epidurals, or c/s
Neonatal latex allergy – Journal of Perinatology
- Mag bolus given for PRETERM reasons other than preE:
- preterm fetal Neuro protection (cerebral palsy prevention)
- Mag increases risk of both uterine atony & maternal pulm edema. Be conservative with fluids, and have 2nd line uterotonics & TXA available.
- preterm fetal Neuro protection (cerebral palsy prevention)
Magnesium Sulfate Before Anticipated Preterm Birth for Neuroprotection
- Preterm deliveries can be PPROM (Preterm, premature ROM) or PLANNED pre-term deliveries.
- If preterm delivery 2/2 PreE/HELLP – Methergine is contraindicated (HTN).
- In hemorrhage – Can use Hemabate (if no contraindication), and OBGYN can use IU pitocin. Can use TXA if bleeding, and OBGYN can use B-lynch suture for uncontrolled bleeding, and insert misoprostol & JADA or BAKRI device post-op
- Generally pregnancies are carried for as long as possible to improve fetal viability, unless mom’s health is at risk. Planned Pre-term deliveries are often for MATERNAL SURVIVAL. If Mom is intentionally delivered pre-term, usually means MOM IS NOT IN GOOD SHAPE. eg:) Severe PreE, HELLP, Cardiac dysfunction, placental abnormality, liver disease, etc, etc. Carrying pregnancy further is unacceptably high risk and detrimental to mom’s health.
- CAN BE VERY HIGH RISK MOM
- Generally pregnancies are carried for as long as possible to improve fetal viability, unless mom’s health is at risk. Planned Pre-term deliveries are often for MATERNAL SURVIVAL. If Mom is intentionally delivered pre-term, usually means MOM IS NOT IN GOOD SHAPE. eg:) Severe PreE, HELLP, Cardiac dysfunction, placental abnormality, liver disease, etc, etc. Carrying pregnancy further is unacceptably high risk and detrimental to mom’s health.
- In hemorrhage – Can use Hemabate (if no contraindication), and OBGYN can use IU pitocin. Can use TXA if bleeding, and OBGYN can use B-lynch suture for uncontrolled bleeding, and insert misoprostol & JADA or BAKRI device post-op
- If preterm delivery 2/2 PreE/HELLP – Methergine is contraindicated (HTN).
- Pre-term uterus considerations from HEMORRHAGE, UTEROTONICS, & LABS page:
- Increased uterine response to oxytocin with increased duration of pregnancy.
- Response increases with upregulation of oxytcin receptor density and sensitivity from 20-30wks, reaches plateau at 34 wks, then uterus becomes even more responsive during labor.
- Very pre-term uterus < 34wks or 2nd TM abortion may have decreased response to oxytocin/pitocin –> methergine may be needed as 1st line uterotonic. (But if induced/delivered early for PreE/HELLP, methergine is contraindicated… womp womp) HTN pt can have IU pitocin, hemabate, TXA, and B-lynch compression suture in hemorrhage.
ACOG 2nd TM abortion: clinical practice guidelines for hemorrhage in pre-term uterus:
Mechanical Stretch Up-Regulates the Human Oxytocin Receptor in Primary Human Uterine Myocytes
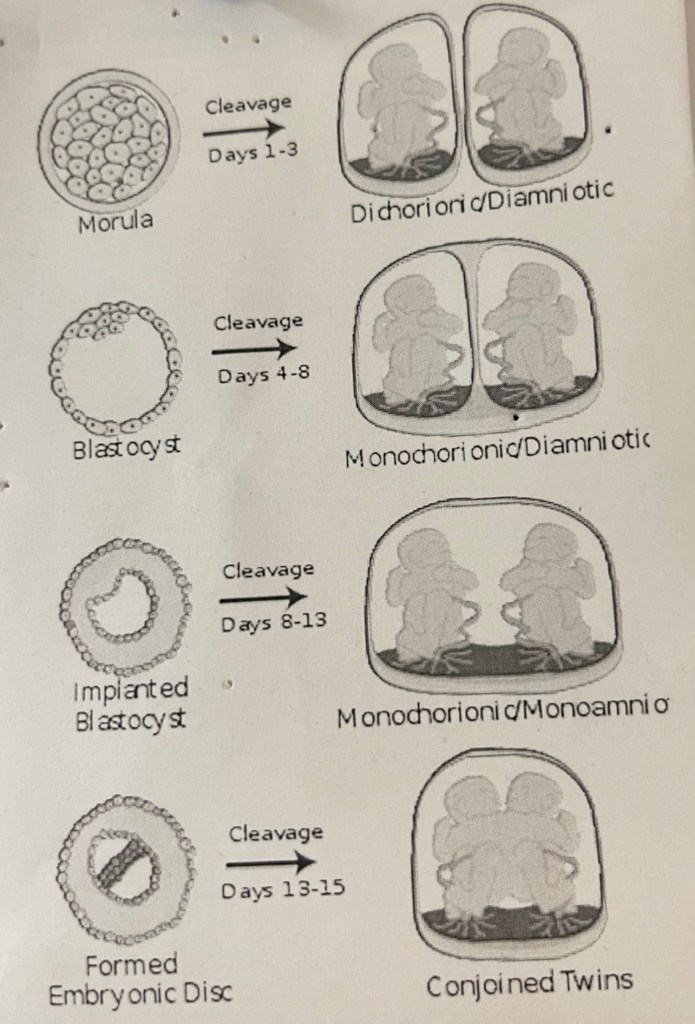
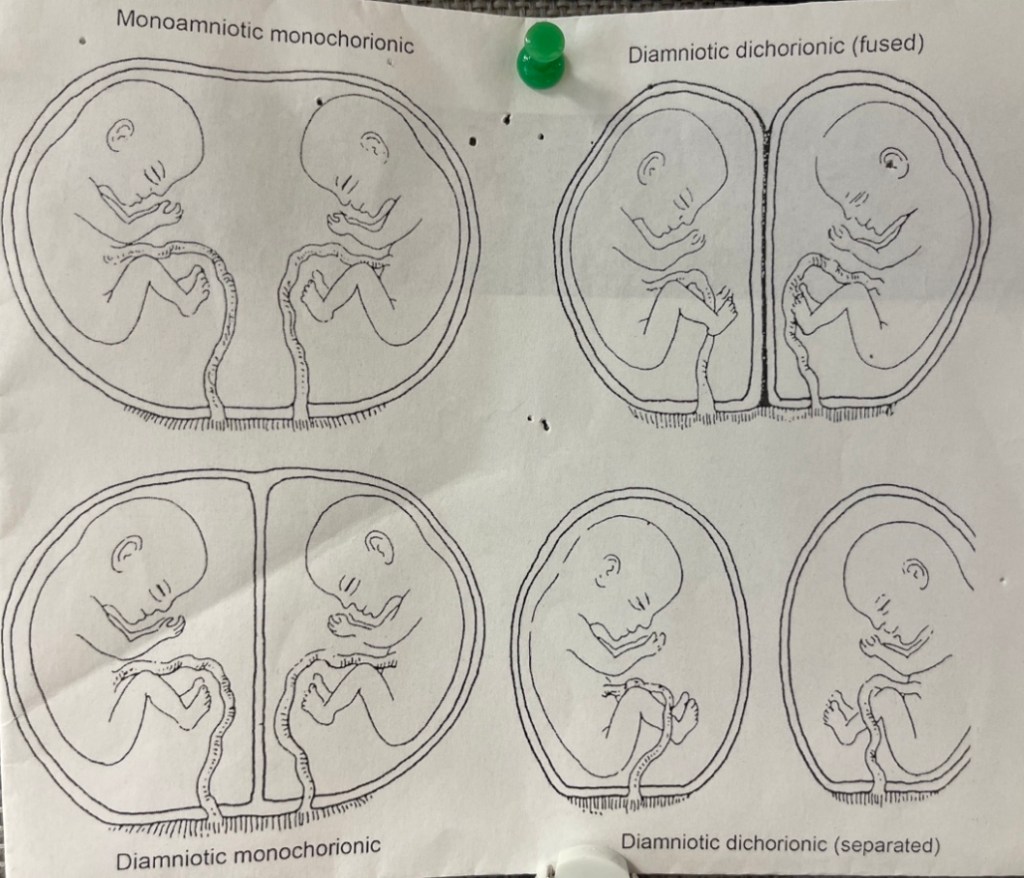
TWIN DELIVERIES:
- IF not a planned c/s, mom labors normally, but twins are DELIVERED IN THE OR (OR3). Mom allowed to labor until ready to push – then whisked to OR for delivery.
- What can happen is: Baby A comes out fine, then Baby B has a terminal decel and we have to emergently section Baby B.
- If no working epidural in place –> GA for stat C/S
- Best to have working epidural in place on labor floor before mom delivers – then the epidural can be emergently dosed for a c/s should Baby B need it, and we avoid GA.
- Labor CSE may not be ideal for this pt – needs a PROVEN, working epidural we can emergently dose for c/s if needed (*although no research actually shows increased incidence of failed epidural conversion with labor CSE, and this is purely my own superstition – so by all means do your thing if you’re a big labor CSE fan)
- Extra stretched uterus of twins/multiples increases risk of hemorrhage.
- If pre-term, consider additional uterotonic concerns re: reduced oytocin sensitivity & responsiveness of pre-term uterus.
- If IVF pregnancy – risk factor for accreta